







INTERVIEW – In countries which restrict access to abortion, MdM is lobbying legislators and in the field with women and doctors.

On a global scale, the right to abortion is not acquired, far from it. Each year, 50,000 women die after an “unsafe”, clandestine abortion. While no country formally prohibits it, many will only tolerate voluntary termination of pregnancy if the woman’s life is in danger.
In these states, associations work to strengthen women’s access to their rights, including the most restricted, and, overall, to improve their sexual and reproductive health.
This fight, Médecins du Monde has been leading in Peru, Haiti and in French-speaking African countries for two years. In parallel with its health and community action, the NGO is trying to convince the governors to move the lines of the right to abortion in their country. Suffice to say that this lobbying activity is delicate, as explained by Anne Sinic, advocacy officer for MdM.
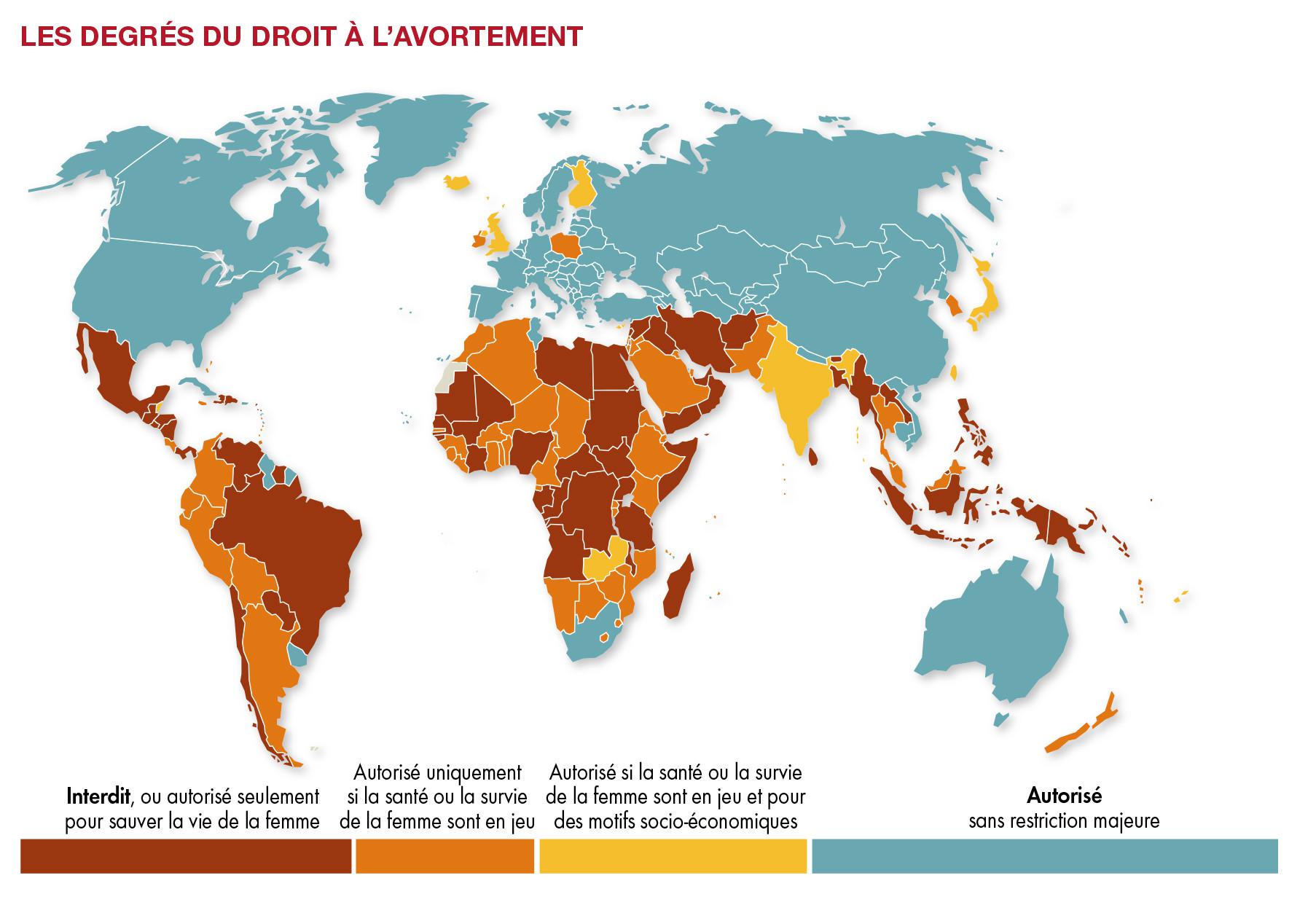
Source: World Atlas of Women, Ed. Otherwise – Huffington Post
Do prohibitive states accept the presence of MdM on their territory?
Anne Sinic: Yes, because all of them have ratified international conventions to this effect. We rely on the MdM network already installed in these countries, to which we are adding this activity. It is a balancing act that requires finesse. Our role consists in particular of reminding legislators of their commitments and responsibilities vis-à-vis these conventions and treaties.
For this we use our network of parliamentarians, we find allies within the ministries, we discuss with all the people likely to have a capacity of influence (United Nations agencies, donors …)
Of course, the changes are subtle. We have succeeded in including the question of the right to abortion in the political agendas of certain States. But we will need more time and more resources to achieve very concrete results, even if the progress is already positive. Two years, in terms of advocacy, is very short.

Anne Sinic, advocacy officer at Médecins du Monde: “ We organized a conference in May in Paris on the right to abortion. We invited African parliamentarians, who, on their return, really contributed to moving the debate forward. . “
How do you manage to improve the right to abortion?
Anne Sinic: We always work in accordance with the local legal framework, which requires a very detailed knowledge of the laws. But it should be understood that the law is not the only obstacle to access to abortion. There are a number of flaws, which we must first detect, before seeing how we can work against what the legal context allows to do.
The barriers are primarily socio-cultural. In these countries, abortion is strongly stigmatized – this refers to the place of women in society. There are a lot of taboos around her sexuality and her body; her decision-making power is weak, she cannot make her own choices when it comes to her health and her sexuality. It also refers to religious brakes, which make women come to be a mother first and foremost. These stigmas are very important determinants in access to abortion.
The law is not everything. We notice, for example, that the medical power can be an important limit. Doctors are also imbued with these socio-cultural representations, which they will carry over to their practices and their discourse, even though the legal framework would authorize abortion. In fact, even if the law changed in these states, this would not immediately allow effective access to abortion.
Anne Sinic, advocacy officer at MdM: “ In South America, a woman who miscarries can be prosecuted. But everywhere, if you have the money, you can end a pregnancy without risk. “
So it is at the level of socio-cultural representations that you act?
Anne Sinic: This is one of the axes of our action. On the one hand, we work with women and health professionals to strengthen knowledge of their rights and duties in terms of abortion. The approach is global, we discuss the issues of contraception, pregnancy, sexuality. We explain to young girls their rights, we insist on the prevention of unwanted pregnancies and try to make all stakeholders aware of the public health problem of unsafe abortion. We rationalize the phenomenon, document it, quantify it.
On the other hand, we assess the health care offer and support the local health system, according to priority orientations. We see, for example, that a real effort has been made in these countries around the health of women who give birth. Maternal mortality has fallen sharply. On the other hand, in care related to abortion, or post-abortion, the mortality rates do not decrease, so we are deploying our action at this level.
Anne Sinic, advocacy officer at MdM: ” Our approach is not only based on public health, but on rights. We do not impose a Western vision, but a universalist. “
.









{kind=link}